Kidney Patient Information for your CKD journey - from diagnosis upwards.
Whether you have just been told you have chronic kidney disease or you are further along the journey, this hub gathers the practical information that helped patients at Manchester Royal Infirmary most. It is written in plain English by people who have lived it.
What is Chronic Kidney Disease?
The CKD patient journey, explained by patients who have walked it
Chronic kidney disease, or CKD, is a long-term condition where the kidneys slowly lose their ability to filter waste and water from the blood. In the UK it affects roughly one in ten adults, and for many people it is spotted by chance during a routine blood or urine test, long before any obvious symptoms. If you are here because you have just been told you have CKD, or because someone you love has been given that news, our first job is to say this: you are not alone, and this is not the end of the story.
This page is our plain-English guide to the CKD patient journey, from the first abnormal blood test all the way through to life after a transplant.
It is written to sit alongside the excellent clinical information you will already have from the MRI renal team, the NHS, Kidney Care UK and Kidney Research UK, and to answer the quieter questions you might not always feel comfortable asking in a ten-minute clinic appointment.
If you would rather see the journey as an interactive flow chart, our interactive CKD journey tool lets you tap through each stage with medical and patient-voice panels side by side. If you would rather read, keep scrolling.
How to use this page
The journey is broken into eight stages in the accordion below. Tap any panel to open it. Each one has a short medical summary, a patient-perspective note in our own voice, and links to deeper information on the MRIKPA site and to trusted UK sources. At the bottom we answer the questions Manchester patients ask us most often, and we point you to the ways you can reach a real human at MRIKPA if you want to talk.
The CKD journey, stage by stage
If you’ve just been diagnosed, one of the first phrases you are likely to hear from a GP, a nurse or a renal consultant is that chronic kidney disease is a “journey” made up of different “stages”.
It can sound clinical, and a bit frightening, when what you really want is a straight answer.
The reason CKD is described this way is that kidney function tends to change slowly over years rather than all at once, and UK renal teams use five numbered stages, based on your eGFR, as a shared shorthand for where your kidneys are today and what sort of monitoring or treatment is sensible next. The stages are not a countdown.
Many people stay in the same stage for decades, some improve with the right treatment of reversible causes, and only a minority move all the way through to stage 5. Thinking of it as a map, rather than a timetable, is usually a lot closer to the truth.
Tap any stage below to open a short patient-voice summary, the medical picture and trusted UK sources.
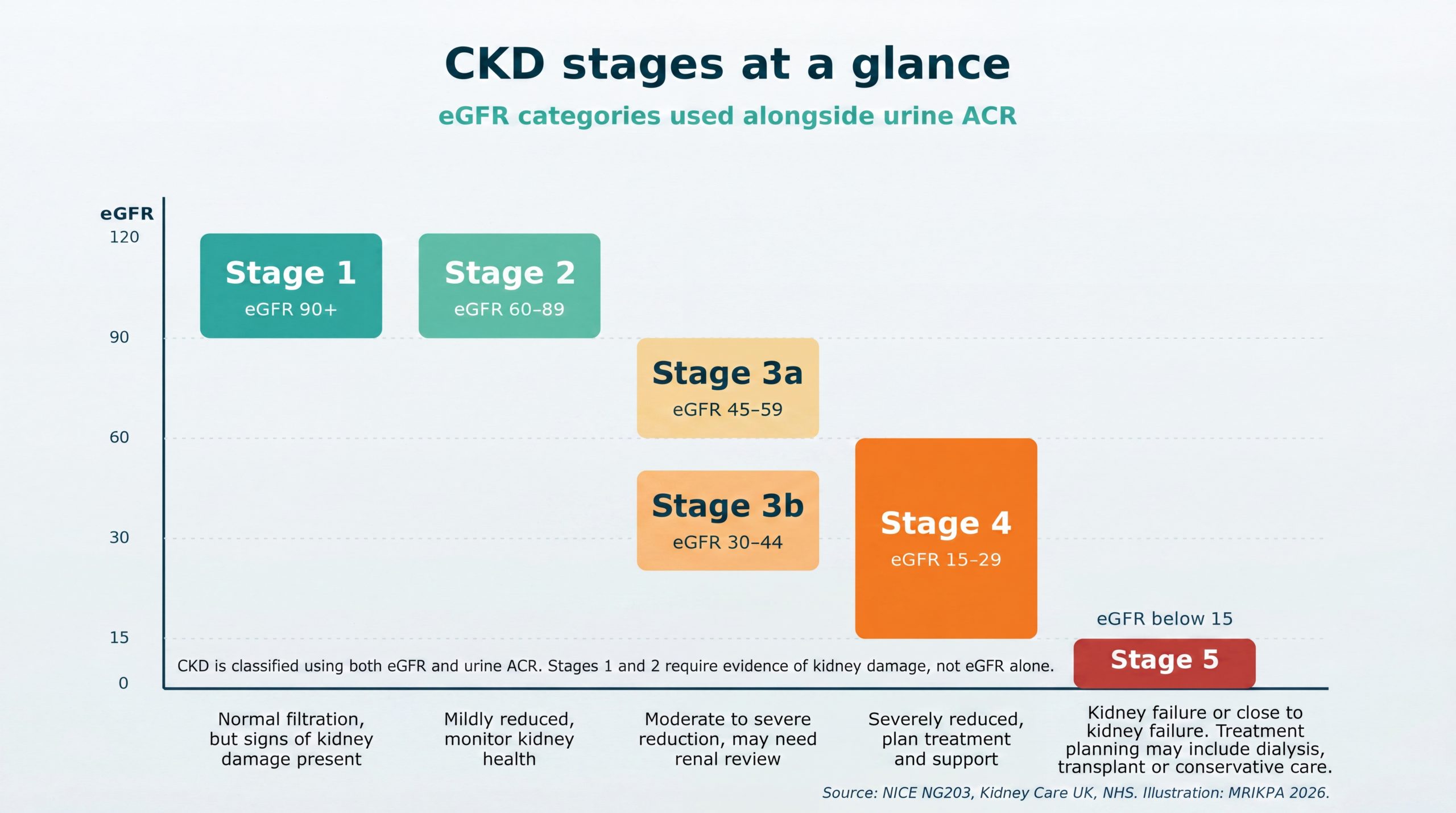
The chart above summarises how CKD is staged by eGFR, and roughly what each stage means for monitoring and treatment. Staging is a guide, not a sentence. Two people with the same eGFR can have very different journeys depending on cause, age, other conditions and how well reversible factors are managed. If your number has just changed and you are worried, the best next step is a specific conversation with your renal team, with a written list of the questions you actually want answered.
At diagnosis: what has just happened?
Most people with CKD are diagnosed through two simple tests: a blood test that measures a protein called creatinine, and a urine test that looks for protein or blood that should not be there. Your GP or consultant uses the creatinine result to work out your estimated glomerular filtration rate, or eGFR, which is essentially a score for how well your kidneys are filtering. A normal eGFR sits around 90 or above. A persistent result below 60, measured at least twice three months apart, confirms chronic kidney disease.
Being told you have CKD can feel like a door slamming. In reality your team is telling you early, so that together you can protect the kidney function you still have. CKD is a spectrum, not a single destination. Many people live full lives for decades at mild stages and never progress.
From a patient point of view, the first week is usually the hardest. You will have questions the clinic did not have time for. Write them down. Bring them to the next appointment. Ask about your exact eGFR number, your urine ACR result, your blood pressure target, and any medicines that might need reviewing. The NHS page on kidney disease is a solid starting point for the medical basics; we have kept our own patient journey overview deliberately short and human for the same first-week feeling.
Stages 1 and 2: early CKD
Stage 1 means an eGFR of 90 or more, but with other signs that your kidneys have been damaged, for example protein in the urine, a known structural problem like polycystic kidney disease, or diabetes-related changes. Stage 2 means an eGFR between 60 and 89 with similar signs. At this point the kidneys are still doing most of their job. You may feel completely well, and you might not need any specific kidney treatment yet.
What matters most at this stage is protecting the kidney function you still have. That means managing blood pressure, looking after blood sugar if you have diabetes, stopping smoking, staying at a healthy weight, and being thoughtful about medicines that can irritate the kidneys, including common over-the-counter anti-inflammatories like ibuprofen. Kidney Care UK’s early-stage CKD guidance is excellent on the day-to-day detail.
From a patient perspective, early CKD is the stage where the lifestyle work pays off the most and the hardest to take seriously, because you feel fine. Our healthy living tips for kidney patients page collects the habits MRIKPA members say have made the biggest difference for them. None of them are dramatic. They are small, steady, Manchester-friendly.
Stage 3: mid-stage CKD
Stage 3 is split into 3a (eGFR 45 to 59) and 3b (eGFR 30 to 44). This is the stage at which many people first meet a kidney specialist. You may be referred to the renal team at Manchester Royal Infirmary or your local hospital for closer monitoring. Regular blood tests will track your eGFR, potassium, phosphate, haemoglobin and bone chemistry. If protein in the urine is high, your team will usually start or optimise medicines that protect the kidneys, such as an ACE inhibitor, an angiotensin-II receptor blocker, or one of the newer SGLT2 inhibitors that are now recommended for CKD by NICE guideline NG203.
Stage 3 is also when tiredness, restless legs, or feeling “not quite right” can first show up. Kidney Research UK’s stage 3 CKD page is a useful readable summary.
From the patient side, this is the stage where our WhatsApp group and our Casual Park Walks become especially useful. You are well enough to live normally, but you have started to realise that kidney disease is going to be part of your life. Talking to people who have already been where you are now helps more than most things. Our Park Walks are gentle by design and built for exactly this.
Stage 4: advanced CKD
Stage 4 means an eGFR between 15 and 29. Kidney function is now significantly reduced, and the chances of reaching kidney failure in the foreseeable future are real enough that your team will start preparing with you. This is usually called “pre-dialysis” or “low clearance” care. You will be seen more often, usually at a dedicated kidney clinic, and conversations about treatment options begin in earnest.
The three broad options are: a kidney transplant, either from a living donor or from the deceased-donor waiting list; dialysis, which can be done in a hospital unit, at a satellite unit, or in your own home; and conservative kidney management, which is supportive care without dialysis, usually chosen by older patients with other serious health conditions. None of these is a failure. They are three different ways to live well with kidneys that can no longer do the job alone.
From a patient perspective, stage 4 is often the stage where we most need other patients. At MRIKPA we match people, informally and confidentially, with members who have been through the same decision. There is no right answer, only the right answer for you. Our renal care at MRI page explains what is available locally.
Stage 5 and kidney failure
Stage 5, sometimes called established kidney failure or end-stage renal disease, is an eGFR below 15. At this level the kidneys can no longer meet the body’s needs on their own and a form of kidney replacement therapy is usually required. The language here is frightening, but the reality is more manageable than it sounds. Many people start dialysis feeling cautiously relieved, because the months before it often involve a creeping fatigue that lifts once treatment begins.
A small number of people reach stage 5 without needing urgent treatment, because they have already had a pre-emptive transplant from a living donor. Others start dialysis as a bridge to transplant. Others choose conservative care. Kidney Care UK’s overview of the stages of CKD is good at making the numbers feel less abstract.
The patient truth is that stage 5 is hard, and it is also survivable, and most people find a routine that works. MRIKPA members who are on dialysis, or who have been transplanted, are some of the most generous people you will meet. They will tell you what nobody in clinic has time to say. Drop us a message via our contact page if you would like to be put in touch.
Dialysis: haemodialysis, peritoneal and home options
Dialysis does the filtering job your kidneys can no longer do. There are two broad types. Haemodialysis pumps your blood through a machine that cleans it, typically three times a week for around four hours per session. It can be done at Manchester Royal Infirmary’s renal unit, at a satellite unit closer to home, or for the right patients in their own home as home haemodialysis. Peritoneal dialysis uses the lining of your own abdomen as a filter; fluid is run in and out through a small tube, either by hand several times a day (CAPD) or overnight by a machine while you sleep (APD). The National Kidney Federation’s peritoneal dialysis guide is a practical read.
Vascular access matters. For haemodialysis this is usually an arteriovenous fistula, made by a small operation several months before dialysis is expected to start. For peritoneal dialysis it is a soft catheter in the abdomen. Your team will plan this well in advance so that dialysis can start smoothly when it is needed.
From the patient side, choosing a modality is one of the most personal decisions in the whole journey. Haemodialysis at a unit gives you structure and a friendly team around you. Home dialysis, whether haemo or peritoneal, gives you flexibility and freedom for work, travel and family. There is a cost of living alongside either, and a MRIKPA member who has already chosen is often the best person to talk to. Our about dialysis page goes deeper into the day-to-day of each option.
Kidney transplant
A kidney transplant is the treatment most people consider the gold standard for end-stage kidney disease, because a well-functioning transplant can restore normal energy and remove the need for dialysis. Transplants come from two sources in the UK: a living donor, usually a relative, partner or friend, or a deceased donor through the NHS organ donor register, managed by NHS Blood and Transplant.
Getting onto the transplant list involves a thorough assessment: heart and lung tests, cancer screening, dental and skin checks, blood group and tissue typing. The wait for a deceased-donor kidney varies, but it is typically measured in years, which is why pre-emptive living-donor transplants, done before dialysis starts, are so valuable when they are possible. Across Black, Asian and minority ethnic communities the wait is often longer because fewer donors come forward, which is why community-led conversations really matter; we keep a page on organ donation in BAME communities as a starting point.
The patient truth is that a transplant is a second chance, not a cure. It comes with lifelong immunosuppressant medicines, regular clinic visits, and careful attention to skin cancer screening, blood pressure, and bone health. It is also, for most recipients, life-changing in the best way. Many of our members have completed in the British Transplant Games after recovery; that page is a good window into what life after transplant can look like.
Life after transplant and longer-term living with CKD
Life after a successful kidney transplant tends to settle into a new normal within a few months. The first year involves frequent clinic visits and blood tests as your team fine-tunes your immunosuppressant doses. After that, most recipients settle into a routine of less frequent monitoring, an emphasis on healthy eating, activity, sun protection, and staying up to date with vaccines. A transplanted kidney does not last forever, but with good care many kidneys function well for 15, 20 or more years.
For those who do not have a transplant, long-term life on dialysis is equally real and equally full. Working patterns, travel, hobbies and family life can all be adapted. The NKF’s haemodialysis treatment frequency guide and Kidney Care UK’s information on managing symptoms are both worth keeping bookmarked.
From the patient side, the long term is where MRIKPA earns its keep. Kidney disease can be lonely. Renal clinics are busy, friends and family can struggle to understand the tiredness or the diet, and life carries on regardless. Our Casual Park Walks, our WhatsApp group, and our members’ events are built to make sure no Manchester kidney patient has to do this alone. If you are newly diagnosed, or ten years into dialysis, or five years post-transplant, the welcome is the same.
What do the kidneys actually do?
Most of us go through life with only a vague idea of what our kidneys actually do, until something draws our attention to them. They sit tucked away at the back of the abdomen, roughly level with the bottom of the ribcage, one on each side of the spine. Each one is only about the size of a clenched fist, yet between them they process around 180 litres of blood every day, every single day of your life. When people talk about “kidney function“, this quiet, round the clock filtering job is what they mean.The kidneys do far more than just make urine. They are the body’s master chemists.
- They remove the waste products left over from food, medicines and normal muscle activity.
- They keep the levels of salt, potassium, calcium and phosphate in balance, so that your heart beats steadily and your bones stay strong.
- They fine tune how much water stays in the body, which is why they play such a big role in blood pressure.
- They release a hormone called erythropoietin that tells the bone marrow to make red blood cells, which is why anaemia and tiredness are so common when the kidneys are struggling.
- They activate vitamin D into the form the body can actually use.
- They help regulate the acid balance of the blood.
When all of this is working well, you never notice. When it begins to slip, the effects can show up in surprising places, from itchy skin to restless legs to breathlessness walking up the stairs.
Understanding this broader job description matters, because it helps make sense of why the renal team tests so many different things at clinic, why blood pressure and diet advice are given the same weight as the eGFR number, and why protecting the filtering units you still have is the single most useful thing you can do at every stage of CKD.
Our diagram shows the headline version of the plumbing. The paragraph below it zooms in on the tiny filter units inside each kidney where the real work happens.
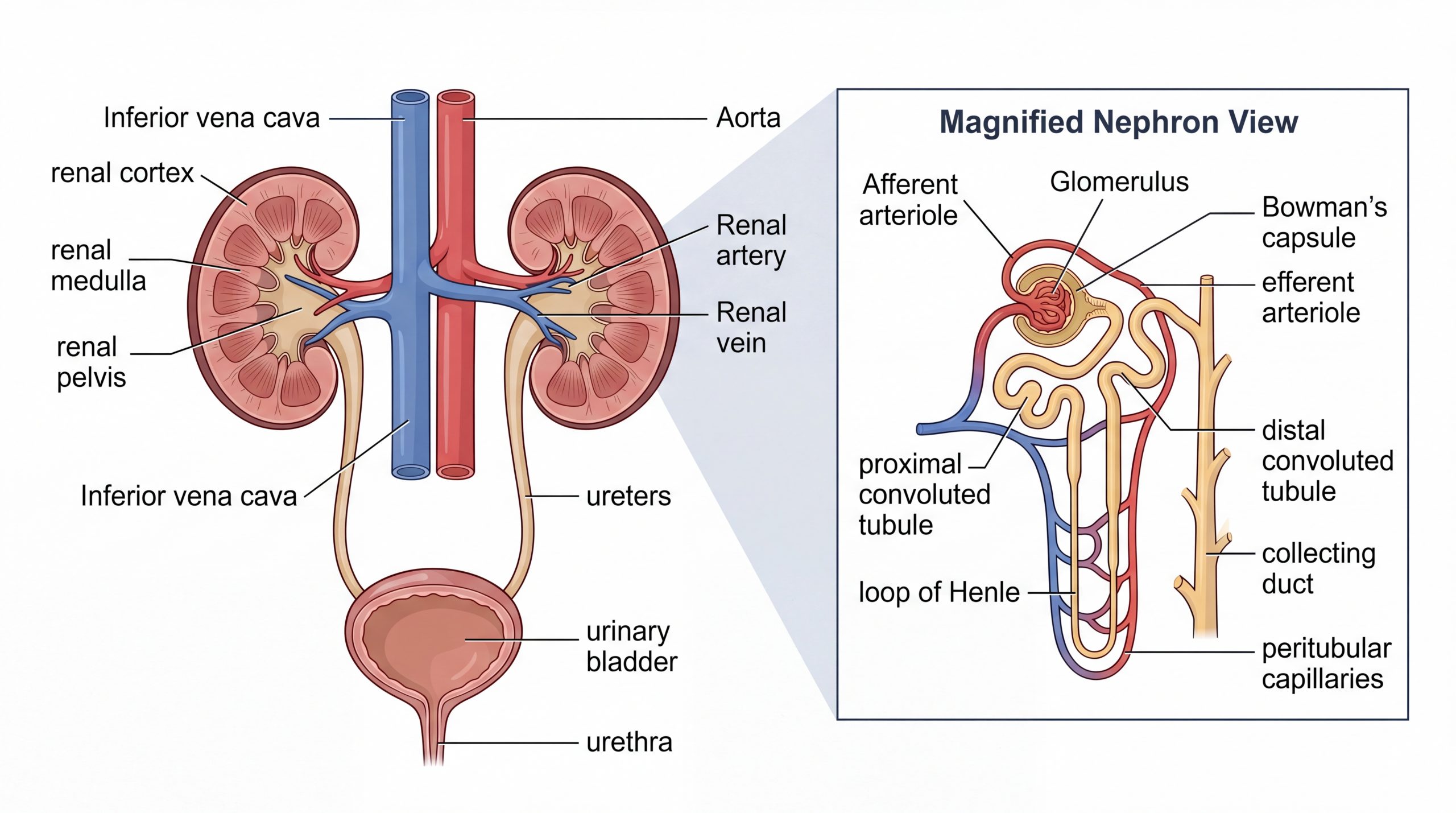
A simplified view of the urinary system.
Each kidney contains around a million tiny filters called nephrons. They clear waste and excess water from the blood and send it to the bladder as urine. In chronic kidney disease some of these filters are damaged and cannot be replaced, which is why protecting the ones you still have is so important at every stage.
Questions fellow kidney patients ask us most
Will my kidney disease definitely get worse?
Not necessarily. Many people with early CKD stay stable for decades, particularly if blood pressure, blood sugar and lifestyle risks are well managed. A falling eGFR year on year is a signal for the renal team to look closely at the cause, the medicines, and any reversible factors. Stability is a realistic goal and, for many of our members, it has been the reality.
What is the difference between eGFR and creatinine?
Creatinine is a waste product your muscles make. Your kidneys remove it. If creatinine rises in the blood it is a sign the kidneys are not clearing it as quickly as before. eGFR (estimated glomerular filtration rate) is a calculation based on creatinine, age and sex that gives a more useful picture of kidney filtering capacity. Kidney Research UK’s eGFR explainer is very good on the detail.
Do I need a special diet?
Not everyone with CKD needs a specialist renal diet. In early stages a heart-healthy Mediterranean-style diet, with attention to salt and portion sizes, is usually enough. At more advanced stages your renal dietitian may ask you to watch potassium, phosphate or fluid intake. Our diet tips for CKD patients page collects the practical Manchester-friendly advice we have gathered from members.
Can I still work, travel and have a family?
Yes. People work full-time on home dialysis. People travel on holiday with unit haemodialysis organised in advance. People have children before, during and after transplant, with careful planning with their renal team and obstetrics. Life does not stop; it reshapes. Kidney Care UK’s travelling with CKD hub is a good practical start for holidays.
What support is there for carers and families?
CKD affects the whole household. Our resources for carers page is written for the people who drive to dialysis, cook for the diet, worry in the waiting room, and hold the family together. You are part of the MRIKPA community too.
How do I speak to someone at MRIKPA?
The quickest ways are to email support@mrikpa.org.uk, to call or text 07745 242 684, or to come to one of our Casual Park Walks. We aim to reply to emails within two working days. Everything you share with us is treated in confidence.
Where to go next on the MRIKPA site?
This page is a starting point.
When you are ready for more, our interactive patient journey tool walks you through each stage with a medical view and a patient-voice view side by side.
Our about dialysis page goes into the day-to-day of unit, home and peritoneal dialysis. Our diet tips and healthy living pages collect the small habits our members say make the biggest difference. For a view of local NHS care, see renal care at Manchester Royal Infirmary.
A word from MRIKPA
If you are reading this in the first few days after diagnosis, please keep one thought: you are one of many, not one alone. MRIKPA has been at Manchester Royal Infirmary since the early ’80s. We have members who have been on dialysis for thirty years and members who were transplanted last month. Between us we have walked every part of the journey on this page, and we are here for you.
The best way to join the community is to become a member (membership is free) or to come and say hello at one of our Casual Park Walks. If you would rather talk quietly first, email support@mrikpa.org.uk or leave a message or text 07745 242 684.
A warm welcome is waiting from people who have walked this path themselves, right here in Greater Manchester.
This page was written by MRIKPA volunteers in April 2026, reviewed for accuracy against NHS, NICE, Kidney Care UK and Kidney Research UK guidance. It is general patient information and is not a substitute for advice from your own kidney team. If your symptoms change or you feel unwell, contact your renal team or 111.